What follows is a workshop I presented at CAST Canada’s Grounding Trauma: Challenging Paradigms conference on April 18, 2018. I’ve included the outline here and the body of the paper is after the cut.
Opening
Introduction
Stage One: Contextualizing the Rise and Role of the Medical Model
Further Contextualization 1: The Neoliberal City
Further Contextualization 2: Municipalities “Curing” Homelessness with the Housing First Model
Further Contextualization 3: Maslow’s Hierarchy of Needs
Stage Two: Exploring Belovedness and Community-Actualization with and among People experiencing Poverty, Oppression, and Housing Deprivation
(A) From Maslow’s Hierarchy to a Siksika Tipi
(B) Housing First within the Context of Housing Deprivation
(C) As Beloved Amongst the Beloved
(D) Mino Bimaadiziwin and the Flourishing of Life
Stage Three: Success and Failure at the Resource Centre
Kindness and the Trauma of Love:
Developing Community in Social Services Increasingly Dominated by a Medical Model of Care
OPENING
Boozhoo. Dan Oudshoorn nidizhinikaaz. Zhaaganash endaaw (Dutch, Scottish, and British). Askunessippi ndoonji. London ndinda. Anishinaabe, Haudenosaunee, Lenape, Wendat, Attawandiron Aki. Mizhiike Minisi. I begin by acknowledging the land where we have gathered. When I speak of the land, I mean the earth and air and water and all of those who are made up of these things and who belong to the land. From the animal nations to the plant nations to various nations of people, including past and future generations, we are all a part of the land. The land does not belong to us – we belong to it. However, when it comes to these specific territories, we do not all belong to the land in the same way. Therefore, I wish to especially acknowledge the Anishinaabe who have belonged to this land for thousands of years. I lift my hands to them for the ways in which they have cared for the land in a way that contributed to the flourishing of life in great diversity over many centuries. I also lift my hands to them because they have allowed me and my children to live, work, and play in their territories. Onishishin.
As a Settler, I benefit from the ongoing project of settler colonialism as it plays out in the occupied territories named “Canada.” Indeed, it is necessary to acknowledge from the beginning that as a white settler of Christian European descent, I am a beneficiary of the genocidal process of colonization that has secured for me legal rights, access to wealth and education, and political and social status. So, it is with a sense of my own liability, accountability, interconnectedness, and responsibility, that I express my thanksgiving and lift my hands to the caretakers of the land I occupy. Chi-miigwetch.
That said, I am concerned that acknowledgments like this coming from people like me frequently only operate as a balm to a guilty settler conscience and do little to contribute to decolonization, the recognition of Indigenous sovereignties, and the restoration of right relationships between various peoples and nations. This is why I opened in Anishinaabemowin. One of the important things about learning languages is that it decolonizes concepts, and frames the world, including one’s self, in critically different ways. If we are to learn to develop life-affirming and life-giving communities in our work, then decolonization is a task that Zhaaganashag must engage. The Anishinaabe belong to this land but my people have come to this land like an invasive species. If we are not to destroy everything, we must learn the words, and thoughts, and ways of the land. I hope that what follows contributes to that process. Miigwetch.
INTRODUCTION
In this workshop, I want to ask questions related to how we go about shaping our communal life together. How do we create spaces dedicated to developing our relationships with one another as members of a shared community? Who is welcomed as contributing and formative members? Who is excluded either partially or fully and why? And do seemingly useful, charitable, or beneficial models of care also serve less obvious disciplinary roles by enforcing mainstream standards upon marginal populations or those considered threatening to the common good? In order to go about exploring these questions I will proceed in three stages.
In the first stage, I want to examine how the medical model of care has gained a hegemonic position within social services and what the implications of that are for communities governed by that model. I will highlight three contemporary and related factors. These are: the rise of the neoliberal city; municipalities pushing to “cure,” homelessness with the Housing First model; and social services ranking needs based upon Maslow’s hierarchy. Here, I will argue that an economic model that prioritizes increasing profit margins, wherein people are valued only to the extent that they are able to sell their labour, contribute to the economy, or accumulate private property and wealth, currently determines how we go about structuring our life together. People who refuse to live in this way, or who are incapable of adhering to these communal values, are branded as ill and as a threat to the health of the community as a whole. Therefore, healing them (and protecting the health of the whole) means providing them with the discipline and assistance needed in order for them to become (re)incorporated into this vision.
In the second stage, I will explore an alternative way of structuring our life together. In contrast to the dominant uses of the medical model of care, I wish to propose an anti-oppression model of mutual trust, respect, care and collaboration with people experiencing oppression. Oppression dehumanizes the oppressor as much as it dehumanizes the oppressed, but in different ways. While the oppressed are dehumanized because they are never admitted into the community of those considered fully human who may enjoy a long and happy life, the oppressors are dehumanized because they live a vampiric existence premised upon stealing land, children, sustenance, health, and life from others. Oppressors, however, tend to be blind to these dynamics and are easily susceptible to ideologies that justify their privilege. Consequently, it is the oppressed who often show us all the way forward. Thus, I believe that it is those whom we label “sick” who are often best equipped to guide us towards communal “health.” To heal, we must realize that it is actually our current way of structuring life and death together that is making people ill.
Finally, in the third stage, I will evaluate some of the successes, challenges, and failures associated with my own efforts to try and implement this kind of community development work in my most recent workplace, a resource centre that focuses upon being a safe, welcoming and useful community space to people experiencing poverty, housing deprivation, oppression, illness, and criminalization. The community members at this resource centre are generally those who have been kicked out of other public spaces (like parks, bus shelters, and street corners) or shared corporately owned spaces (like malls and libraries) and who have also been banned, barred, or suspended from other social services (like shelters or drop-ins). They are labeled by others as “too violent” or “too psychotic” or “too noncompliant,” to be welcomed elsewhere. As this section makes clear, I do not wish to pontificate as an expert but, rather, I come as a fellow traveler seeking to share and learn from you as much as I’m sure you all have come to share and learn from others.
STAGE ONE: CONTEXTUALIZING THE RISE AND ROLE OF THE MEDICAL MODEL OF CARE
When considering the rise of the medical model, the first thing to realize is that this is a relatively recent phenomenon. Medicine used to be practiced very differently, health and sickness used to be understood very differently, and medical practitioners had a very different place in the social hierarchy. So, what happened? How did the discursive practices of health care come to dominate all others?
I believe what happened was this: from the Renaissance onward, there were dramatic shifts within Western societies. Science, empiricism, and rationalism, confronted the worldview provided by the dominant Christianities. This confrontation created a crisis in authority for those who were able to legitimately wield force over others within society.
Specifically, the dawning of the age of scientific reason, created a crisis for those who had used religious discourses to justify the deployment of force to defend contemporary distributions of wealth, property, and power. If deviant people are not witches, sinners, and heretics, by what right can those in centralized places of power use force in order to ensure that the status quo continues to serve their interests? How can the use of force be justified and be made to feel right, appropriate, and acceptable? With the decline of religion and the rise of reason, a vacuum of legitimacy appears here.
Monarchs and the aristocracy experienced this crisis most desperately as their power was intimately connected with the church. Hence, revolutions accompany the rise of reason. As monarchs fell, others rose and it is ultimately the capitalist class who seized power and began to accumulate the greatest fortunes. Their new found wealth, paired with shifting beliefs, allowed the capitalists to control and modify institutional power. Christendom was replaced by the nation state and feudalism gives way to capitalism. The question facing the capitalists was how they could justify using the kind of force necessary to maintain their massive fortunes. It is this crisis of legitimacy that is resolved by the rise of medicine and the discourse of public health.
In order to understand how this occurs, it’s useful to provide a brief history of the notion of mental illness. Here, I draw from Michel Foucault’s History of Madness, and Deviance and Medicalization by Peter Conrad and Joseph Schneider.
Foucault argues that Western society is unique in understanding “madness” as “mental illness.” How did this happen? Well, Foucault says, as reason replaces religion, behaviours that were previously classified as sinful came to be seen as “folly” or “unreason.” Behaviours that were classified as deviant were reclassified as sickness – illness, in other words, followed after a predetermined badness.
Thus, by the mid-1600s, large institutions of confinement were built to house those labeled as fools. These institutions housed the unemployed, criminals, paupers, and people considered mad. Here, the primary markers of madness were poverty, unemployment, and idleness. It was important to the emerging capitalist class that madness be associated with these characteristics. Their rise to power required an easily exploitable and docile base of workers. Beggars, idlers, and paupers were seen as embodying a threatening model of communal deviance that needed to be broken up.
Here, the mad are not yet considered sick. They are viewed more like animals, controlled by passions. However, fear began to spread that such people were contagious. So, a reorganization took place to address those fears – those who could work were sent to workhouses, those who were criminals were sent to prisons, and those who remained “mad” were sent to newly founded insane asylums. This reorganization came along with the recognition that poor people were actually beneficial to the wealth capitalists because they created a pool of surplus labour that could be used to keep workers in line – if workers threatened a strike, or wanted an increased share in the profits derived from their labour, they could be replaced by others from this standing reserve. Consequently, people experiencing abject poverty were reintegrated into society precisely as people experiencing abject poverty and were then maintained by charity in order to function as an ongoing threat to any kind of organized labour.
Within the insane asylum itself, the cure for madness continued to be seen as having patients accept the morals, values, and priorities of bourgeois society. Special attention was given to obedience, work, and the value of property. Sanity came with learning to judge these things in the same way as others.
Much of this trajectory continues until the 20th-century when major developments in psychotropic medications increased compliance in deviant groups without also severely limiting their functionality. The (no longer mad or insane but) mentally ill, then, no longer need to be isolated but can be (re)integrated into their proper place in society. However, this shift in the location of those who are mentally ill – from institutions to the community –has led to a massive expansion in community based mental health programs now required to maintain social order. A shift in the definition of “health” has been a critical component of this. Previously, health was defined as “the absence of disease” but now health is defined by a comprehensive list of biopsychosocial determinants. Thus, the World Health Organization asserts: “health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” and health includes “healthy or unhealthy behaviours.” Essentially anything can be considered a health determinant. The medical model is now distributed through all areas of life – it has successfully replaced religion as the moral compass of society and the tool by which force can be brought to bear on the lives and bodies of potentially anyone, anytime, anywhere.
However, we must remember that what has often been medicalized and treated is simply deviance – “behavior that is negatively defined or condemned in our society.” Furthermore, given the rise of neoliberal capitalism, deviance has also been redefined in economic terms – as living in a way that negatively impacts somebody’s profit margin or that is costly to the State. In this context, the medical model is a perfect tool to facilitate social control because it claims to be rooted in the objectivity of science and evidence-based studies, hiding the fact that moral decisions and judgments are being made, and that violent or coercive actions are being taken.
One of the consequences of this is that there are right and wrong ways to be sick. If a person is sick the right way – i.e. if they see that being sick is undesirable and try to recover, if they agree to cooperate with a treatment or recovery plan assigned by the appropriate authority – then that person is exempted from normal responsibilities for a set period of time. However, if a person is sick in the wrong way, if they do not prioritize spending most of their waking hours working a bullshit job in order to give money to a landlord to rent a shithole apartment in a house they could never afford, and if the sick person refuses to express remorse or take full responsibility, and refuses to express gratitude to the parties who line up to get them back on track, then the sick person can expect to be punished – dropped by social workers, discharged from shelters, targeted by police officers, and institutionalized in jails or psychiatric wards.
Normalizing both surveillance and a certain way of seeing (“the medical gaze”) helps to accomplish this. To explore this, I want to outline two more texts by Foucault: The Birth of the Clinic and Discipline and Punish. In The Birth of the Clinic, Foucault talks about how the appearance of medical clinics, changed the ways in which medicine was practiced and the ways in which people chose to view themselves. Through the clinic, a medical gaze emerges that views people as individual and unique collections of symptoms – the individual becomes the portrait and seat of disease. Hence, managing disease, especially epidemics, was as much about managing people and social spaces as it was about treating illness.
Three things should be emphasized. First, health care is dominated by a gaze that transforms a person into an individualized and objectified seat of disease. Second, as Foucault shows, this continues to be motivated by class-based interests. Third, because the individual is the seat of the disease, it is the diseased individual who becomes the threat to the status quo. Consequently, the medical gaze is focused heavily upon the person, who is deviant precisely because he or she is diseased. Everything about that person must be examined and purified. Surveillance advances to accomplish this.
In Discipline and Punish, Foucault examines the rise of prisons in order to explore surveillance as a sociopolitical phenomenon. Over against prior practices of public torture, Foucault argues that prisons were created not to “punish less” but in order to “punish better.” As this shift occurred, it was largely poor people who were criminalized. The bourgeoisie were especially concerned with maintaining their property and those who did not have enough to survive, who get away with committing small property related crimes under feudalism, were now confronted with the full force of the Law. Guilty person go from being made into a public spectacle, to being removed from society in order to be reeducated and corrected. Within the prison, the guilty person must be disciplined into penitence. He or she must learn to be subjected and docile and must learn to be economically productive while being politically obedient. Hence, prisons become both Correction Centres and Penitentiaries.
However, it was the invention of the panopticon within the prison system that revealed the true efficacy of surveillance.

The panopticon was a prison that had a central tower looking out on the cells arranged in a ring around it. The people in the cells were always in sight of the tower, but they, themselves, could not see into the tower. This state of conscious and permanent visibility, produced a self-disciplining population. Because they thought they were always being watched, prisoners were far more obedient. This model of self-disciplining through ubiquitous surveillance then became the desired standard for general society. If you can produce people who make themselves compliant, then you are able to present yourself in a more humanitarian way. Plus, this saves a lot of money.
It is the medical model that justifies the dispersal of this panoptic gaze into all areas of society. Public health lingo is used to justify interventions that would otherwise appear to be coercive or violent. Thus, for example, in many programs, social service workers have far greater access than the police do to the homes, lives, and private spaces of people. Within the evaluations of these workers, any perceived maladjustment signifies illness. Successful conformity signifies that the person is now healthy.
Those of us working in social services are on the frontlines of this. We collect massive amounts of data related to the lives of populations that are considered threatening to the status quo. There is no area of life that we do not watch over. As proof of this, simply review questions asked on forms like the Global Appraisal of Individual Needs Short Screener (GAIN-SS), the Ontario Common Assessment of Need (OCAN), the application forms for subsidized housing, or the Admission and Discharge Criteria Assessment Tool (ADAT).

These assessment tools demonstrate how the medical gaze operates. Many of us could answer a lot of the questions in a way that would be perceived of as problematical – maybe we’re lonely. Maybe we don’t really feel a sense of satisfaction in life. Maybe we’ve experienced childhood trauma. Maybe we struggle with eating regularly and keeping our house clean. Maybe we feel like it’s impossible to determine if our way of viewing things is realistic. However, we are all functioning just fine – specifically, we are going to work regularly and paying our rent and mortgages. We are doing what people at our socioeconomic level are supposed to do. And so we’re not asked to complete these surveys. Because it is not so much how you answer these questions that shows there is something wrong with you – it is the fact that you have been selected to be asked these questions in the first place that shows there is something wrong with you.
Further Contextualization 1: the Neoliberal City
Now, if this exposition of the class-based moral force undergirding the medical model of care helps us to understand how it rose to an hegemonic position within social services, it is equally important to observe how the transition from post-war Keynesianism to neoliberalism within urban centres across Mizhiike Minisi, has altered the reasons why this care is forcefully brought to bear upon the bodies and communities of people experiencing poverty. Within the neoliberal city, wherein government understands itself to be less concerned with caring for people and more concerned with paving the way for free markets dominated by real estate developers, fierce competition within housing markets, gentrification, and the so-called revitalization of urban cores into hubs for tourism, consumption, and innovative business, the medical model becomes the tool used to justify the destruction of communities of people experiencing poverty and community spaces dedicated to those people.
In this way, Neoliberalism mirrors Canada’s brand of settler colonialism, only instead of Europeans colonizing Indigenous territories, we now see rich people colonizing poor neighbourhoods (Indigenous peoples continue to be over-represented). While Christianity and the white man’s burden were previously used to justify this act of colonizing a land that was said to be left wild, neglected, and in a state of abandon or disrepair (as per the legal doctrine of terra nullius), now the discourse of public health is used to justify the takeover of inner-city communities which are pictured as rundown, boarded-up, or totally neglected (even though most of the boarded up buildings have been purchased by real estate developers who deliberately permitted them to fall into ruin). Thus, just as so-called Indians were believed to be incapable of properly caring for or owning land, so now members of poor communities are considered illegitimate inhabitants of their own spaces. They must be removed. One way of accomplishing this is by shifting funding priorities in order to annihilate spaces designated as community spaces. This happens in a few ways. First, many traditional drop-in centres are defunded because they are not viewed as contributing to desired outcomes related to housing, health, labour readiness, or financial independence. Second, the drop-ins that continue to exist are re-oriented around producing specific outcomes – that is to say, drop-ins are no longer places where people can come to be or hang out or spend time with friends but, instead, become places where people sign in and out in order to attend particular groups, often oriented around things like recovery, life skills, CBT, DBT, personal health, resume building, and so on. While this kind of transition is good for producing stats that align with the goals of government funders in a very competitive market, it also raises barriers to service – excluding those who are either unwilling or unable to participate in such groups, despite ubiquitous claims to “client-centredness” – and it also transitions a community space into a more clinical or performance oriented space – i.e. precisely the kind of space where many of those who used to attend the drop-in have encountered violence and been made to feel unwelcome.
This work has been facilitated by scare-tactics related to whatever illicit drug is currently said to transform people into dangerous, psychotic, monstrous beings. Thus, a considerable amount of ignorant fear-mongering around Crystal Methamphetamine, cloaking itself in the objective discourse of a medical science, has contributed to social services adopting an extremely reactive stance regarding staff and client safety and has produced the closure of low-barrier community spaces.
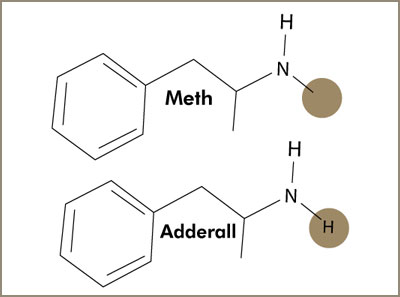
Of course, given that Crystal Meth is essentially indistinguishable from Adderall, and given that Adderall is prescribed to millions of people across Mizhiike Minisi, what all the hot workshops about biochemistry and meth are neglecting to mention is that one could make equally scary presentations about almost any drug or even about the risks, long term adverse health outcomes, and changes to our brain chemistry, that occur when we engage in daily activities like driving or sitting looking at a computer for an extended period time. Understanding the connection between Crystal Meth, violence, and harm requires situating that discourse within a conversation about criminalization, prohibition, colonization, and housing deprivation. If not rooted here, the medical model of care is too easily deployed for other ends and meth scares are used to support neoliberal gentrification projects—just as crack scares and Nixon’s “war on drugs,” were used in racist assaults upon black communities from the ‘70s through the ‘90s, and just as the equally racist concept of “reefer madness” was pimped by law enforcement agencies in the ‘30s and ‘40s to massively increase police budgets and jurisdictions. We’ve seen this kind of fear-mongering cloaked in the language of medical science many times before.
Thus, whereas during much of its early history, the primary purpose of the medical model of care was to produce a compliant and effective labour force, within neoliberalism it is also used to justify hostile takeovers of communities wherein pre-existing inhabitants are forced to migrate elsewhere. These forced migrations are fracturing community-destroying events. People move as small family units or as individuals and so a way of structuring life together, the way developed by the people in the community before the neighbourhood was taken over, is destroyed and people are forced to either develop new relationships and integrate into mainstream ways of structuring life together, or end up homeless, in prison, or dead.
Further Contextualization 2: Municipalities “Curing” Homelessness with the Housing First Model
The way in which numerous municipalities have adopted the Housing First model as their self-professed “cure” for homelessness illustrates this well. Housing First is hot with municipalities, first and foremost, because it tells them they can save a lot of money if they start trying to house people instead of funding other social services, like shelters, which are now said to be simply “warehousing” people. Furthermore, not only will a lot of money be saved as neoliberal cuts to social services are pursued but these very cuts can be presented as a philanthropic act rooted in noble intentions and supported by empirical, evidence-based research.
Housing First operates from five central principles: (1) Immediate access to housing with no housing readiness conditions; (2) Consumer choice and self-determination; (3) Recovery orientation; (4) Individualized and person-driven supports; and (5) Social and community integration. When all five of the principles are respected and implemented in a program wherein workers have manageable caseloads, very good housing outcomes frequently result and many people who are considered “chronically homeless” have been “successfully housed” over the medium to long-term. So what’s wrong with this? Well, a few things.
First, because funding for social services is limited, and because new cash isn’t going to be injected to fund Housing First programs, cuts are made to other services in order to produce funding. Again, services oriented around developing or affirming the community and networks of support that exist amongst people experiencing poverty are usually first on this chopping block. Also on the block are services that are said to be warehousing people and, indeed, cities have learned that they can reduce their homeless counts simply by cutting the number of shelter beds available – thus, budget cuts to shelters make it look like Housing First is having an immediate positive result, when really many people have simply joined the so-called “hidden homeless” in squats or couch surfing or have gone back to abusive partners. Most cities seem to see this as acceptable as they compose lists of “the most expensive homeless people in the City” (based upon number of 911 calls and frequency of E.R. visits) and focus on housing those people.
Secondly, as Sam Tsemberis himself has recognized, municipalities that implement the Housing First model within a plan to end homelessness tend to put a lot of pressure on service providers to produce numbers that show they are meeting this goal and so corners invariably get cut. Specifically, principles #2 and #5 tend to be neglected. Given that Housing First workers seek to integrate clients into market housing, they do so by developing relationships with specific landlords at specific locations. Clients are then pressured to move to these locations rather than being able to choose the community or neighbourhood in which they would like to live. Furthermore, these locations are often in neighbourhoods far removed from spaces and people familiar to the clients. This is so for three reasons: (1) market rates for rentals are lower in neighbourhoods far removed from the urban core; (2) the neoliberal city wants people living in poverty to move out of the core; and (3) clients are deliberately isolated from their friends and their peers because those people are considered obstacles to the successful housing of the clients. Thus, long-term friends and those who have helped people negotiate and survive multiple traumas over several years are considered “negative influences.” They are said to enable self-harming, unhealthy behaviours. Thus, the fifth principle of Housing First, pushes for social and community integration into mainstream society as a replacement for the social networks and communities it helps to destroy. However, this principle is also often neglected as workers find it both difficult and time-consuming, and have large caseloads of clients to get housed to meet the City’s goal. Therefore, when Housing First is implemented in this way, many people end up going back to the streets and neighbourhoods that are familiar to them. Given ever expanding case loads, I have seen Housing First programs quietly discharge people from the program immediately prior to people losing their housing in order to manipulate their stats. This also stops workers from being required to engage in the time-consuming and often impossible task (given the realities of market housing and their limited connections) of engaging in the suggested rapid rehousing of those who are “hard to house.” However, of potentially even greater concern is the number of people whom I know who died shortly after being housed in a Housing First program. I was struck by the significant number of “chronically homeless” people who died within the first year of being housed when London first began to pursue this model. I was also struck by how the dataset did not track these deaths but, instead, had recorded each dead person as successfully housed long-term.
Strictly from a cost-saving perspective, this is true.
Further Contextualization 3: Maslow’s Hierarchy of Needs
Finally, I want to point out how tools and paradigms that we take for granted in our work contribute to this. Here, I wish to explore the utility of Maslow’s hierarchy of needs.
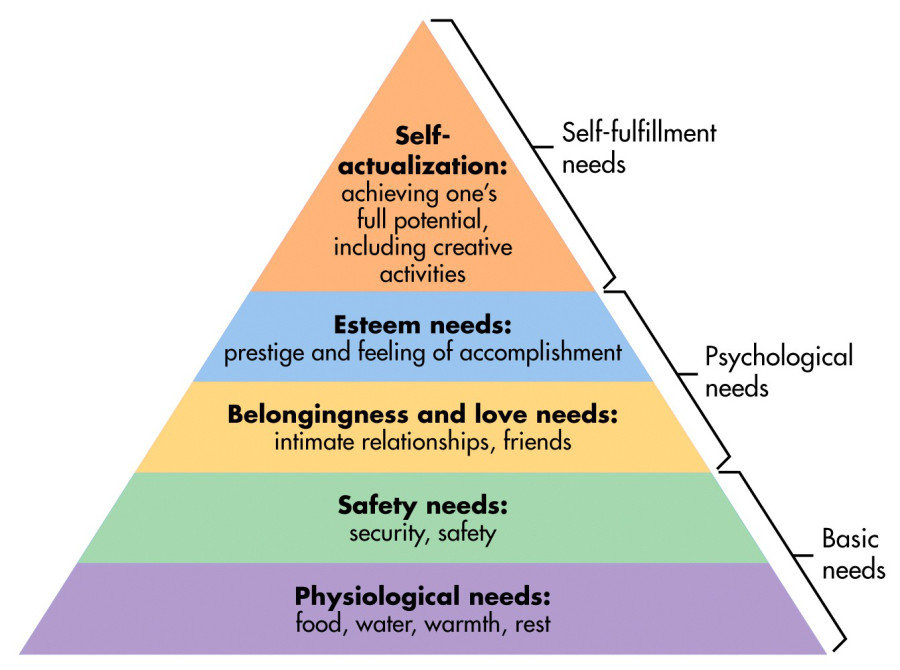
Abraham Maslow posited that human needs were something like a five-tiered pyramid with physiological needs being at the base, followed by needs related to safety, then needs related to love and belonging, then needs related to esteem and, ultimately, at the top, self-actualization needs. The bottom two layers are considered “basic needs,” the middle two layers constitute “psychological needs,” and the apex pertains to “self-fulfillment needs.” Now, according to the medical model, the higher the level of need, the less important meeting it becomes. There are pragmatic reasons for focusing on lower level needs – it is easy to generate datasets related to things like food and housing and then demonstrate that one is meeting related goals. It is also easy to do this in a quantitative way that meets the standards of evidence-based research rooted in the Eurocentric patterns of power/knowledge that we refer to as scientific. It is much harder to do this with a person’s sense of belonging, with their sense of respect for others, or with the ways in which they inhabit a moral discourse that relates to their sense of self-fulfillment. Thus, the medical model of care may confidently say a lot about meeting individual physiological needs, but the higher we go up the hierarchy, the more vague, uncomfortable, and unfunded the discourse becomes. Consequently, services focus upon “basic needs” and argue that this is morally justified because basic needs are the very base of the pyramid.
However, this pragmatism is not politically innocent and, depending on one’s perspective, it is not as morally justified as it might appear to be. For one thing, remaining focused upon “basic needs” ensures that services view people experiencing poverty, oppression, or housing deprivation as isolated individuals. This depoliticized social work focuses upon producing better biopsychosocial health outcomes within an individual rather than deconstructing the socioeconomic and juridico-political structures that are responsible for producing, poverty, oppression and housing deprivation in the first place. More than that, however, this use of Maslow’s hierarchy also reinforces the belief that meeting higher level needs is optional and, therefore, according to the logic of the free market, something that is only available to those who can afford to meet them. It is as if people must prove their ability to meet their basic needs before they graduate to being recognized as the kind of person who can then have legitimate higher level needs. In this way, the use of Maslow’s hierarchy actually reinforces dehumanizing stereotypes about oppressed peoples whom we call sick, as though they are less-than the rest of us who are very much focused upon self-actualization and who can afford to pay private therapists to help us. However, even when it comes to higher level needs, Maslow’s focus remains upon the individual – how do love and belonging meet the needs of the individual. And all of this is bound by the timeframe of the individual’s life. There is little sense of connectedness to past generations or of commitment to future generations . There is little sense of accountability, responsibility, interconnectedness or belonging-together-with others. Thus, if I used the example of colonialism to talk about neoliberal approaches to urban centres, here the social services end up looking like the Jesuit shock troops who proceeded the arrival of the government agents – despite possible good intentions, they destroy pre-existing community models, narrow the focus to the individual, and then integrate that individual into a new way of sharing in life and death together.
STAGE TWO: EXPLORING BELOVEDNESS AND COMMUNITY-ACTUALIZATION WITH AND AMONG PEOPLE EXPERIENCING POVERTY, OPPRESSION, AND HOUSING DEPRIVATION
In stage one of my argument, I moved from the large to the small. In this stage, I will go in the opposite direction. I will begin by exploring a Siksika alternative to Maslow’s hierarchy. I will then talk about reframing our conversation about housing in terms of housing deprivation as a form of death-dealing oppression. I will then explore Jean Vanier’s and Henri Nouwen’s ideas about being beloved members of a beloved community as an alternative to the vision of the neoliberal city, and I will conclude by looking at Nishnaabeg visions pertaining to the art of living the good life as an alternative to the values that currently structure our communal life together.
(A) From Maslow’s Hierarchy to a Siksika Tipi
One of the fascinating things I learned while looking for an alternative to Maslow’s hierarchy is that Maslow actually developed his model while doing anthropological research on a Siksika reserve. However, while his model is inspired by Siksika teachings, Maslow produced a considerably different product given his own biases and rootedness within Eurocentric traditions. Cindy Blackstock – a member of the Gitxsan Nation and the Director of the First Nations Child and Family Caring Society – explains how the Siksika model differs from Maslow’s.

First of all, Blackstock says, this triangle is not a pyramid. It is a tipi. As such, it is solidly rooted on the earth but its tip reaches the skies. Hence, the earthly and the heavenly are understood to be united. In this united whole, the top is just as fundamental as the base. Not only this, but self-actualization, which Maslow places at the top of his pyramid, is at the base of the Siksika tipi. The trajectory, then, is one that moves from self-actualization, to community-actualization, to cultural perpetuity. This actualization is understood in an holistic manner that incorporates all elements of a person – the physical, emotional, mental, and spiritual. It is especially related to what the Nishnaabeg refer to as nwenamdanwin (choice-making) and ndendowin (responsibility-taking). However, the individual is not taken in isolation but is positioned in relation to others, including both past and future generations. Hence, nwenamdanwin and ndendowin are connected with aabawaadiziwin – togetherness, or the art of being together in right relations with others. Thus, one gets a sense for a radical respect for the freedom and autonomy of individuals, but one also sees how free and autonomous people, who are confident in their sense of who they are, also come together to form communities that meet the needs of all members and that seek to do so over time and in balance with other beings. Of course people still need to eat and have access to shelter but, at the core, this model is about understanding one’s place in the space-time material and spiritual world(s). This is the basis upon which community-actualization takes place. This community-actualization, in turn, supports cultural perpetuity. It supports the maintenance over time of socioeconomic, cultural, and political structures that contribute to the flourishing of all life.
Much of this is lost when we focus on being able to statistically track the ways in which we meet the basic needs of individuals in order to demonstrate that our services are saving money for the cities in which we work. In this regard, Craig Willse’s comments about the biopolitics of understanding “the homeless” as a population to be managed are instructive. In The Value of Homelessness, Willse notes how pushes for mass data collection and integrated databases have produced a supra-personal entity known as “the homeless population” and that this entity, how it is understood, how it changes, how it is managed or reduced, becomes the primary focus of government funded programs. From this perspective, communities that have developed among people experiencing poverty, oppression, or housing deprivation are considered problematical or toxic, and individuals themselves are reduced to boxes that can be ticked in order to show that the government is getting the best bang for its buck. However, if we want to engage in the kind of work where we don’t simply view people as components of a population that needs to be managed cost-effectively but, instead, if we wish to acknowledge the sacredness, beauty, goodness, and loveliness of all people, I’d like to suggest that we start thinking about how to organize community development around the Siksika tipi instead of Maslow’s hierarchy.
(B) Housing First Within the Context of Housing Deprivation
Here, I would like to return to my comments about Housing First and the limits it faces to being successful other than as tool for managing a population and reducing municipal costs. I would like to suggest that what is fundamentally missing from those advocating for this solution is an understanding of homelessness as form of oppression that we can refer to as housing deprivation.
In the International Covenant on Economic, Social and Cultural Rights, the General Assembly of the United Nations recognized that adequate housing is a fundamental human right. Canada has ratified this. Housing First attempts to recognize this in some ways. However, as any survivor of domestic violence knows, a house is not a home and much of how Housing First is unrolled is premised upon first severing people from relationships and community spaces where they feel at home. Again, if we are to draw parallels between this work and Canadian efforts to colonize and assimilate Indigenous populations, it is no wonder that Housing First programs often fall apart at the community integration stage. To the shock of settlers, not everyone who is Indigenous wants to become like settler Canadians. And to the shock of the rich, not everyone wants to become assimilated into a society or labour force dominated by their wealth. Indeed, when I look at the before and after photos that agencies who claim to serve “the homeless” sometimes put out as a part of their marketing campaigns, I’m hard-pressed to see how they differ from before and after pictures of Indigenous children sent to residential schools.


So there are two points I want to make about oppression here. First, Housing First often operates in a community-destroying way. Second, Housing First never challenges the oppressive nature of housing markets, property accumulation, and sky-rocketing rental prices that ensure that some people are deprived of housing. Here, again, Willse is useful. Willse talks about housing as “a thing that makes live and lets die.” In his words, “a house is a technology for the organization and distribution of life, health, illness, and death.” Within our contemporary context, housing deprivation, then, is better understood as a social phenomenon than an exclusively individual experience. As a social phenomenon, housing deprivation “is produced to make literal room for the speculative urban consumer economics of neoliberal capital.” Contemporary discourses around housing and homelessness, then, naturalize and perpetuate what is essential a death-dealing form of oppression related to housing. In fact, Housing First is premised upon developing good relationship with the very developers responsible for transforming our cities in this way, and it is seen as an alternative to other more expensive – but internationally more effective – long term solutions like investing in safe affordable social housing, co-ops, RGI-housing, or rent controls. Thus, while Housing First may be useful in removing some of the more costly homeless folks from the streets, it does nothing to prevent ever greater numbers of people from ending up on the street in coming years. Therefore, if we want to do more than simply reduce costs or reduce harms, if we want to actually uproot the causes of harm and begin to structure our life together in a fundamentally different way, then we need to be operating from an anti-oppression stance.
(C) As Beloved Amongst the Beloved
One way of moving into an anti-oppression way of thinking and acting, is to orient ourselves around acknowledging, honouring, and celebrating the belovedness of all people, especially those whom others have treated as though they are not beloved or as though they are worthless, bad, broken, sick, and appropriate targets of State-based violence. It is love that opens us up to the other and it is also love that opens us up to being more self-critical and reflective about our participation in services or programs that we perhaps mistakenly assumed were ever only good or noble or caring. It is also love that opens people up to self-actualizing in ways that they find delightful. It is coming to know ourselves as beloved that can be the greatest and most powerful trauma of living. There are two things I wish to emphasize about this.
First, I wish to emphasize that while experiencing love from other’s can be critical to transitioning to a true awareness of one’s self as beloved, a mature knowledge of one’s self as beloved is not dependent upon experiencing or receiving love from this or that person. Ultimately, when one knows oneself as beloved, this is embraced as an identity, as the core of who one is, and while this may be affirmed or challenged by others, it remains who one is regardless of any other experiences. I am beloved because I am lovely. This is what I am.
Second, I very deliberately refer to experiencing love in this way as a kind of trauma. Here, I want to appeal to Judith Hermann’s definition of trauma. In Trauma and Recovery, she states the following:
Psychological trauma is an affiliation of the powerless. At the moment of trauma, the victim is rendered helpless by overwhelming force… Traumatic events overwhelm the ordinary systems of care that give people a sense of control, connection, and meaning… Traumatic events are extraordinary, not because they occur rarely, but rather because they overwhelm the ordinary human adaptations to life.
In other words, what makes trauma traumatic is the way in which it overwhelms us and makes it impossible to believe things we used to believe about ourselves or the world in which we live. When we are traumatized, we are left in a devastated and unrecognizable landscape even though everything still looks the same. Now, what I think trauma studies tend to overlook by always focusing on trauma as it pertains to negative experiences of violence, terror, disaster, and death, is that we can also have positive experiences that are just as overwhelming and just as devastating to previously held beliefs. For example, when I was seventeen years old, I was kicked out by my parents and was deprived of housing. At that time, I adhered to a deeply entrenched belief that I was a piece of shit, who deserved to be abused. But then I encountered a love where I was known, honoured, celebrated, and delighted in. In my encounter with this love, I was, to quote Hermann, “rendered helpless by overwhelming force” and my way of making sense of myself and the world was also overwhelmed and no longer made sense. I came to know myself as beloved and, knowing myself in this way, also convinced me that belovedness was at the core of who we all are. This then set the course for the rest of my life. Along the way, I have concluded that it is not only the great hurts that can forever change us. Great love can change us just as traumatically – and it can change us even after we have been traumatized by the great hurts.
Helping to awaken this sense of belovedness in others who have been taught to believe other things about themselves, is central to our work. But it is not enough for us to affirm individuals as beloved. We must also work to affirm that they are members of a beloved community and work to encourage the flourishing of that community. Here, I think it’s important to remember that Henri Nouwen’s work – which speaks very movingly about our individual status as beloved – is first and foremost rooted in Jean Vanier’s understanding of the need for people to feel a sense of belonging within a community of others who are also beloved and who also belong. Vanier, of course, pursued this by developing the L’Arche community model. In this model, people with various developmental disabilities are not separated from one another or considered a hindrance or barrier to the well-being of one another. Rather, structures are put in place to encourage communities of people with developmental disabilities to share in the fullness of life with one another. And they do. Temporarily able-minded people are simply facilitators and assistants in this project. What I would like to suggest is that we treat this as a model for how we go about trying to assist in the development of beloved communities with and among people experiencing poverty, oppression, and housing deprivation. Rather than contributing to the annihilation of their communities, we should view ourselves as facilitators and assistants, contributing to the community building which is already going on under our very noses although we may be entirely clueless to it because we are tracking and prioritizing the wrong things. We, too, need to be liberated from the medical gaze so that we can properly identify that which is death-dealing and that which is life-giving.
(D) Mino Bimaadiziwin and the Flourishing of Life

This Painting is a Mirror by Christi Belcourt (acrylic on canvas; ~6.5ft x 9ft; used with the artist’s permission)
Finally, pulling back to the big picture level, I want to draw on Leanne Betasamosake Simpson’s discussion about the Nishnaabeg notion of mino bimaadiziwin and how this is collectively pursued in Nishnaabeg culture, economics, and politics. The term mino bimaadiziwin refers to the good life or the art of living the good life, the way of the good life. Mino bimaadiziwin is both a means and an end. It is not simply an idea or concept or value or name but it is, more fundamentally something active and refers to life together being creatively structured and practiced in a certain way. Now, there are a number of complexities here, but Simpson argues that mino bimaadiziwin essentially comes down to living in a way that acknowledges, values, honours, respects, celebrates, affirms, and contributes to life in all of its diversity and flourishing. This embraces individual lives, all kinds of life, and the interconnectedness of all life. In this way, the Anishinaabe, i.e. the good people, live the good life.
Currently, Canadian settlements are not communities structured around love, mutual care, or the flourishing of life in all its diversity, richness, and abundance. Even the so-called “caring professions” operating in this context are far from this and are lost in funding proposals, competition, surveillance, discipline, punishment, and a Darwinian struggle for brand recognition and equity. If we are to change this then, collectively, we have to start asking the kinds of questions I have tried to ask in this workshop. We can also try to start mapping ways forward in our own contexts, and, in the final part of this workshop, I wish to examine one effort to do this and how it both succeeded and failed.
STAGE THREE: SUCCESS AND FAILURE AT THE RESOURCE CENTRE
In the Spring of 2012, I began working at a resource centre in London, Ontario. I moved to London from the downtown eastside of Vancouver, where I both worked and lived as a member of the community. The downtown eastside was the most loving community-oriented place I have ever lived. As an example of this, consider a sting the RCMP set up there. In the summer of 2015, an undercover officer posed on a street corner as “disabled and brain-injured” person in a wheelchair. On his lap, he had an unzipped fanny pack with money spilling out of it. He wanted to catch some robbers. And what actually happened? Over a number of days many community members approached him and gave him free food and more money, they told him where the shelters were, and they asked if they could help him. On multiple occasions, known gang members approached him and told him to zip up his fanny pack so that he didn’t get robbed. One drug dealer went so far as to zip up his fanny pack for him. Nobody robbed him or harmed him. To me, this encapsulates both the kind of mutual care that defined that community and the stigma that outside groups brought to bear on the community when they tried to enter into it.
So I experienced some culture shock when I moved to London. People experiencing poverty and oppression in London seem far more colonized at the level of their outlook and self-understanding than many in Vancouver.
So, I had a lot to try and figure out as I began working at a resource centre as a part of a local community mental health program. This program claimed to be oriented around harm reduction, client-centredness, and psychosocial rehabilitation but this claim was more rhetorical than actual. In fact, the program rented space within another organization that zealously enforced abstinence. Consequently, if people wanted to access the resource centre, they had to first clear the barriers of admittance to this other service, and people banned from accessing this other service could not access the resource centre. This other service was also for men only and so any who did not identify as male were unable to enter. On top of this, I had problems with their staff members barging into the resource centre to bully or intimidate community members whom they appeared to personally dislike. The primary groups being offered were all twelve step programs.
Initially I tried to engage this environment by starting a new group called the London Shelter Residents Advocacy Group. In this group, I encouraged what Paulo Freire calls a process of conscientization. Conscientization is designed to help people to transition from viewing themselves as powerless to understanding themselves as active agents in both their personal lives and within the broader socioeconomic and political milieu. This group was initially very successful. Shelter residents began to learn their rights for the first time, they began to familiarize themselves with grievance processes, and they engaged in a successful campaign to have one of the local shelters renovate its bathrooms. These bathrooms were among the most disgusting I have ever seen. Clients had complained for years but their complaints had been ignored or brushed aside with references to budgetary constraints and other priorities. All of this changed once people became organized, gathered evidence, and threatened to go external with pictures that were taken. Suddenly, money appeared and the bathrooms were renovated. However, the local shelters and the City Manager of Homeless Populations viewed the success of this group and the way in which it was attracting a growing membership as a bad thing. It challenged their budgets and it also forced them to engage things that were priorities for the clients rather than allowing so-called client-centred agencies to determine what everybody’s priorities should be. Consequently, my boss told me I would no longer be permitted to facilitate this group and, given that it was still very new, it soon fell apart.
So, I began to reevaluate what I had learned about the people whom I was trying to serve. Recognizing that London had a significant number of people drinking alcohol that was not intended for consumption, I did two things. First, knowing that many of these people were not interested in 12 step programs, I trained to facilitate SMRT Recovery groups to offer a recovery model oriented around empowerment. Second, I started an Illicit Drinkers Support Group that was not oriented around recovery at all but that was a safe, community space for sharing and support amongst people who drank in this way. Two things put an end to these groups. First, most of the people in the Illicit Drinkers Support Group died and, instead of drinking hand sanitizer or Listerine, more and more people were using meth as the cheap alternative to other substances. Second, in my third year in the Resource Centre, the staffing level was reduced to one person and operating the space alone, which was accessed by 50-85 people per day, and which I wanted to be as accessible to as many people as possible, meant that I stopped running groups.
By the end of that solo year, I saw an opportunity to try and make a move to create a much lower barrier community space oriented around meeting the self-identified needs of people who were being excluded from other services. I proposed hiring another staff member and moving the resource centre to a space that had opened up that was ideally situated to permit access to anyone, without fear of being hassled by neighbours given that it had a discrete backyard and was bordered by an empty parking lot and railroad tracks. Additionally, this space will able to provide a free computer lab, free wifi, bathrooms with showers, a kitchenette, and free laundry services. My proposal was a success, the move took place and, in the Spring of 2015, another staff member was hired. Thankfully, I was very lucky and we found a truly wonderful person to help develop community in the resource centre. She has contributed a lot, both to the centre and to my own development as a person and I am deeply saddened that she was not able to join us today.
Initially, after moving, there was considerable pressure to run groups and workshops. This is largely because stats from workshops are an important source of data for securing funding. I was accustomed to regularly consulting with clients in terms of program development and priorities, and I did this with developing workshops. I also built collaborations with other agencies who were best equipped to meet self-identified client needs. Yet, it became persistently obvious that the community members whom the resource centre was seeking to serve were not going to spend much time attending workshops, even if those workshops were geared towards areas of interest or need that they identified.
We needed to go back to basics. The people we were trying to serve had been so abandoned, betrayed, abused, and harmed by institutions and programs that were supposedly there to care for them, that we had to tangibly demonstrate that we actually cared for people in ways that made people feel cared for. We had to ensure that we were a safe, welcoming, and useful space and were experienced as such by the clients who accessed the space. Deploying the tools and perspectives already mentioned was critical to this. But these things had to be demonstrated in tangible ways. Thus, for example, when our toilets clogged, I didn’t simply lock the bathrooms and wait an hour or two for a janitor to come and take care of them. Given that many community members were allowed nowhere else with a washroom, this would have forced people to go to the bathroom outside. Instead, I got the plunger and took care of the clogs myself. This showed community members that I did not think I was better than anyone else, I did not pass gross work onto others, and I was willing to do what needed to be done in order to make sure clients continued to have access to spaces that mattered to them. This was a very successful tactic.
However, one of the first things we needed to do to ensure the safety of the space was take care of the police. The program that used to operate in the space where the Resource Centre was located, as well as other programs that used the same building at different hours, operated within a “you scratch my back, I’ll scratch yours” relationship with the police. Staff members regularly violated client confidentiality, and allowed police officers who did not have warrants and who were not in fresh pursuit to access their private property, databases, and program spaces. Some even called police to report people who were breached. In return, the police were expected to come quickly when people from these programs called 911. Therefore, when the Resource Centre moved to the new location, we had a problem with police officers driving into our lot or coming into our building to bully or intimidate clients. These officers also expected me to disclose confidential information to them. I refused to do this. I explained that I was a LIHN-funded community mental health program and that client information was protected by the Personal Health Information Protection Act and so I could not provide any information. Furthermore, I explained that the program spaces were private property and since they had not been called to be there, had no warrant, and were not in fresh pursuit, they would have to leave. I received two responses to this: first, I became targeted by police officers who became very aggressive with me. For example, one day, after asking an officer to leave, I had six different cruisers individually arrive in our parking lot and each officer took my personal information and said they wanted to see the guy who didn’t want police officers coming around. Later, one of those cruisers drove slowly beside me as I walked home. In fact, this matter of police bullying wasn’t fully resolved until a police officer was caught on camera picking me up and throwing me into a wall because I was politely explaining to him that he was not permitted in the resource center. He and his partner lied about this incident but once the video footage confirmed my version of events, the police backed off.
The second common response I received from officers was threats that they would not respond to 911 calls for help if I didn’t break the rules for them. Mostly, I was okay with this. Given that almost all of our community members had been victims of police violence, I had a firm policy of never calling the police unless I thought someone was at imminent risk of death or very serious injury. Indeed, if we hope to be safe, welcoming, and useful to people who might sometimes engage in activities that have been criminalized and who have almost all been abused by police, then calling the police to deal with conflicts in our community spaces cannot be an option, except in the most dire of circumstances. The police, by the way, did follow through on this threat. Shortly after they threatened me, I called 911 because an acutely psychotic person with a boxcutter was trying to cut up another person. The police, knowing the full details of the situation, took 25 minutes to respond while I looked after everyone’s safety. But that call was one of only three 911 calls made from the resource centre over the course of a year. By way of comparison, a night program that operates out of the same building and that serves many of the same clients, called the police ~122 times in the same time period. Even though they called the police more than 40x more than us, no one was seriously hurt in the Resource Centre that year. Viewing people as beloved, acknowledging and honouring others, and being useful to people in ways that they experienced as useful, significantly aided our ability to mediate and resolve conflicts or comfort people who were upset.
Having demonstrated a willingness to confront police bullying on behalf of our community members, people felt safe and cared for and believed that we wouldn’t rush to implement punitive measures that would cause them harm. This was further affirmed by our willingness to engage, mediate, and resolve situations where other workers would be scared and call the police. This produced very important results: because community members felt this way about us, people were far less inclined to act violently in the resource centre and when some people did begin to become aggressive, their peers were far more likely to engage to successfully comfort them, problem-solve with them, and find nonviolent solutions to their problems. Thus, there are many people who come to the resource centre who are red flagged as armed and very dangerous at services across the city and who have never once acted violently in the resource centre. In fact, they have all contributed to the community in wonderful ways.
A second key tool used to demonstrate we were a safe, welcoming, and useful space, was getting an organization that paid lip service to harm reduction, to actually engage in harm reduction practices. The numbers related to injection drug use in London are pretty staggering and almost all of the regular community members of the Resource Centre inject drugs. London is also undergoing various health crises that jeopardize the wellbeing of street-level injection drug users. Because of this, we created a proposal suggesting that the resource centre become a distribution point for harm reduction material, like safer injection kits. This proposal was a success and created and agency-wide paradigm shift. This program transformation tangibly demonstrated our care to the community members who saw that we were serious about caring in a non-judgmental way that meaningfully prioritized their well-being.
Critical to all of this was prioritizing kindness and gentleness in the context of interpersonal relationships. This is shown in day-to-day small acts of tenderness and affection and, despite pressures from bosses and other who don’t understand the work, having time to just shoot the shit over a cup of coffee, or mop up a mess like it ain’t no thang, or colour or play a game of crib is very important. Responding with intimate concern to people who show distress instead of rushing to enforce rules or reacting out of fear is also fundamental. However, acting with kindness, gentleness, and affection also means challenging and sometimes ignoring or breaking rules that are cruel and unsympathetic. If you’re watching people like a hawk trying to catch them doing something they shouldn’t so that you can suspend them, you are not being affectionate or even psychologically safe. If you see people doing something that is not permitted in the space and you approach them in a non-confrontational manner and don’t draw negative attention to them in front of their peers, and remind them of the program guidelines and talk with them about why those guidelines exist, you are being affectionate. The former approach will encourage a culture of mutual suspicion and hostility. The latter approach will encourage a culture of mutual trust and respect. That said, there are some rules I refuse to enforce. According to the agency I work for, if more than one person goes into the washroom together, then those people are supposed to be suspended for at least 24 hours. However, being aware that many community members have nowhere else to go, being aware that sometimes people need help changing dressings on wounds that are in difficult places, knowing that having a shower together may be the only opportunity some couples have to share a moment of intimacy, and knowing that fentanyl is everywhere and that people who use alone are more likely to die, I categorically refused to enforce this rule. Laws exist to serve people. People do not exist to serve the Law. When Laws become death-dealing, and when we lack the power to change them, it is love that motivates us to break them. This, at least, is the approach I have always taken.
As a result of these things, the number of people accessing the resource centre exploded. Significantly, the vast number of people referred to us, were referred by their peers. They came because they heard that the resource centre was safe and welcoming and that when staff members there helped you, they actually followed through on what they said they were going to do in a prompt, professional, efficient and caring way. In my experience, only a very small percentage of social workers actually work this way. Thus, we gained a reputation for doing things other workers didn’t do, sticking with things until we found a solution, and advocating on behalf of community members with other organizations in ways that other workers were afraid to do. At the same time, this growth was escalated by the closure of at least six other relatively low-barrier community spaces that used to be accessible to our community members. These six spaces closed or significantly raised their barriers due to pressures related to neoliberal gentrification, shifts in funding priorities, and rampant fears related to people who use crystal meth. Increasingly, we became the only low-barrier community space left for people who had been excluded from everywhere else. Thus, whereas our daily numbers at the start of 2015 hovered between 50 and 85 people per day, by the start of 2018, they were up to 110 to 170 people per day. Despite these exploding numbers, and despite making regular requests for an increase in staffing, there remained only two full time staff members in the resource centre, with a third staff member from another program assigned to work occasional hours within the space.
As long as our numbers hovered below 120 people per day, my partner and I found we could still get to know everyone by name, engage in the little but oh-so-meaningful acts of care that built relationships and established the tone and culture that we wanted to guide the space. However, as our numbers rose, as more and more people came to us seeking assistance with individual needs, and as our staff level was not increased, we found we lost the ability to set the tone and establish the core culture and trajectory of the environment. Furthermore, as other agencies began requiring clients to fill out more and more forms to access their services, time spent developing relationships within the community space was often redirected to completing a SPDAT or intake form or whatever else with a community member in the office. As a result, more and more new people, whom we were unable to get to know, began to import cultures and violent practices that they had learned as survival skills in other institutions that encouraged them to act those ways. Consequently, the number of violent incidences or crises we experienced began to increase and, instead of proactively working to create a safe, welcoming and useful community space, we became reactive, hopping form crisis to crisis. This culminated, last fall, in me personally intervening in 13 very violent incidences in a 6 day period. After becoming a father, I have found that I am much more deeply impacted by potentially fatal incidences and, having already come very close to death in a knife fight the previous year, my PTSD was triggered, I had an acute stress reaction, and my doctor ordered me on a sustained medical leave.
After I went on my leave, management increased the staffing level. However, they brought in a team of people who do not value community spaces for people experiencing poverty, oppression, and housing deprivation, who believe they have more important things to do, who are afraid of many of the clients, who understand their role to be that of policing the space, and who see themselves as superior to the community members. Rather than working to mediate conflict and secure the inclusion of all people, punishment and exclusion are becoming the go-to responses to any kind of conflict or perceived disorder. In fact, a full program transformation or closure now feels imminent. This will leave many very vulnerable and truly wonderful people with nowhere safe to go.
This, then, is the rise and fall of the resource centre. I hope that it helps to contextualize the challenges we face when trying to implement the tools and lenses provided here. I use it as an illustration but it is part of my dibaajimowinan and my debwewin – my personal story and my truth. More literally, as my debwewin, it is the sound of my heart. I hope it resonates with the rhythms of your hearts today.
However, I think this helps us to see that, for as long as we continue to focus very narrowly on healthcare as understood by the medical model of care, we will never breakthrough to the kind of life-giving and life-affirming communities we long to be members of. Increasingly, it seems to me, our best efforts to produce the new world in the shell of the old either only end up replicating the old or end up being co-opted and crushed before they can be fully born. Perhaps it is time to explore more confrontational less-legal tactics. How do we go about facilitating squats in empty buildings? How do we help organize with renters to forcibly prevent evictions? How do we disarm the police? How do we share resources with one another in order to maintain our own housing and food stability as we do these things? Maybe these are ways to not only reduce harm but actually confront and begin to tear down the power structures that perpetuate poverty, oppression, and housing deprivation. Because I don’t want to spend my life fighting losing battles in an effort to hold onto a tiny pocket of community space where all people are welcomed and valued—I want a society that looks like that. I want that for my friends, my family, and myself. I want that for all of us. A society structured around wealth accumulation premised upon dealing death to those considered disposable is revolting. Perhaps, then, we to need find ways to revolt. I speak these words as a father, lover, fighter, friend, and brother.
Nii’kinaaganaa. All my relations.
Thank you Daniel for your great presentation at Grounding Trauma last week. It was a pleasure to meet you. I discussed and shared some of your ideas on my self-care (mainly for physicians) Facebook page: https://www.facebook.com/WhileCaringForOthers/
Sending many good wishes for you and your/our human and animal family.,
Hi, Harry! Thanks for your comment and the good wishes. I’m honoured you shared some of this — I post it publicly to try and make it as accessible to as many people as possible and try to do that with most of my papers (instead of, say, trying to submit them to journals which might increase my own brand status but where the content will be hidden behind pay walls). All the best to you and yours.
Reblogged this on The Cloud of Unknowing.